By: Martin G. Brodwin, Ph.D., C.R.C., California State University, Los Angeles
Using the ICF as a guide, counselors in higher education working with students with disabilities can focus more on health and capabilities, placing less emphasis on impairment and limitations. By highlighting positive factors as seen within the ICF model, counselors can more effectively help their students succeed in college and beyond.
The World Health Organization (WHO, 2001, 2015) developed the ICF as a universal system to interface with vocational rehabilitation, return to work, and inclusion and participation in community and society – emphasizing components of health rather than consequences of disability. The aim of the ICF is “to provide a unified and standard language and framework for the description of health and health-related states” (WHO, 2001, p. 3). There are three domains: the perspective of the body, the individual, and the environment (society). The ICF uses a comprehensive biopsychosocial model of disability encompassing a person’s body functions and structures, activities and participation, as well as environmental and personal factors.
There are two prior approaches which came before the biopsychosocial model: (a) the medical model and (b) the social model. The medical model sees disability as a problem of the person caused by disease, trauma, or other health conditions – emphasizing medical care. A person’s disability within this model is considered a deficiency or abnormality. Having a disability is seen as negative; therefore, one is seen as needing a cure to be able to fit into society as much as possible. Control is seen as belonging to the physician (the medical community), not the individual with the disability.
The social (or societal) model sees disability as neutral; disability is viewed primarily as a difference – it is society which disables individuals through designing everything to meet the needs of the majority of people who do not have disabilities. The remedy is to change the interactions between the individual and the environment which requires increasing social interaction, and places the responsibility on society to modify the environment, allowing the person full access to and participation in all aspects of social functioning. Control is seen as belonging to social action to remedy the barriers, not the individual with the disability.
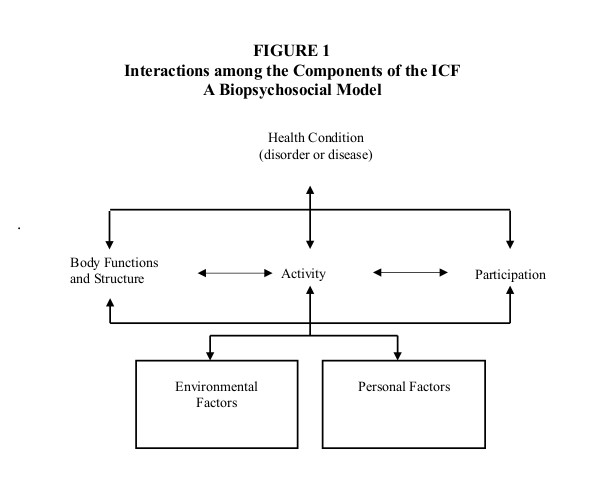
The ICF combines both the medical model and the social model and adds additional concepts. It defines disability as (a) impairments, (b) activity limitations, and (c) community restrictions. To minimize the effects of disability, one needs to evaluate the interaction between the individual with health conditions and personal and environmental factors (Parkin, Corcoran, & Stolfi, 2017). As indicated by these researchers, the ICF biopsychosocial model views disability and disease as an “intricate and variable interaction of three conditions: biological factors (genetic, physiological), psychological factors (attitudes, personality, behaviors), and environmental/social factors (culture, ethnicity, socioeconomic status, beliefs, spirituality).” Environmental factors include such aspects as architectural impediments, social barriers, and poor social support systems. Figure 1 illustrates the components and interactions of the ICF biopsychosocial model.
 “The focus of the ICF is on health and functions that relate to disability, rather than impairment and handicap” (p. 4). The ICF defines key terms in its conceptual framework as follows (WHO, 2001):
“The focus of the ICF is on health and functions that relate to disability, rather than impairment and handicap” (p. 4). The ICF defines key terms in its conceptual framework as follows (WHO, 2001):
Health – components of health (physical or psychological function) and components of well-being (capacity to function within the environment).
Function – all body functions, activities, and participation in society.
Disability – any impairment, activity limitations, or participation restrictions that result from the health condition or from personal, societal, or environmental factors in the person’s life.
Impairment refers to a deviation from certain generally accepted population standards of function.
Individuals react quite differently to the same impairment and, hence, have a different degree of disability. Additionally, the workings of the body can affect the mind, and the workings of the mind can affect the body. An individual may not adjust well to a relatively minor physical impairment, whereas another person is able to excel despite the same impairment. Someone with a major impairment, such as paraplegia, may overcome disability by returning to college and becoming a successful professional, whereas another person with paraplegia may stay at home developing overwhelming depression and anxiety. A person using a wheelchair will find less architectural barriers (eg., stairs) in a well-developed country, whereas in a less developed country, the person may not have accessibility because of a lack of ramps to access buildings. The stairs become the disabling barrier even if the person has a positive attitude. Hence, the connection between disability and the environment.
With understanding and use of the ICF model, higher education counselors can more effectively serve their students. As these students succeed in college, they become more equipped to enter the workforce on a successful career path.
References
Parkin, K., Corcoran, J. R., & Stolfi, A. (2017). Introduction. In A. Moroz, S. R. Flanagan, & H. Zaretsky (Eds.), Medical aspects of disability for rehabilitation professionals (5th ed., pp.1-18). New York, NY: Springer.
World Health Organization (WHO). (2001). ICF: International Classification of Functioning, Disability, and Health. Geneva, Switzerland: Author.
World Health Organization (WHO). (2015). Disability and rehabilitation. WHO Global Action Plan 2014-2021. Retrieved July 3, 2017 from http://www.who.int/disabilities/about/action_plan/en